The incidence of hoarseness in childhood varies between 4 and 23% and occurs depending on the structural or functional problems of the larynx and vocal cord. Voice problems are seen in school age children and boys more. Descriptions of the voice disorder by the family are in the form of hoarseness, change in voice quality, husky voice, cracked voice, weak voice, thin and high-pitched voice, or thickening in the voice.
What are the most common causes of childhood voice disorders?
The majority of voice problems in childhood is caused by misuse such as too frequent or prolonged crying, too loud and shouting speech and harsh speech habits. Misuse or abuse of voice can lead to nodules on the vocal cords (callus in both vocal cords), polyps (unilateral growth on the vocal cord), cysts, some bleeding focuses, and hematoma.
In addition to these, gastric acid reflux, infection of the vocal cords and surrounding tissues (laryngitis), systemic diseases (such as thyroid gland problems), congenital causes (web formation between the vocal cords, vascular vocal cord tumors-hemangioma, vocal cord paralysis-unilateral or bilateral), other benign tumors (such as papillomatosis) and functional voice disorders (muscle tension dysphonia, psychogenic disorders and puberphonia) may also be a cause.
How are childhood voice disorders diagnosed?
The approach to a child with a voice problem concerns more than one section. These sections are primarily Otorhinolaryngologist and later speech-language pathologist, pediatrician, child psychiatrist or psychologist, family members (especially parents) and other departments (such as pediatric gastroenterology, pediatric allergy units).
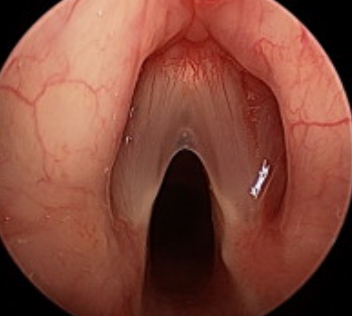
The first step in diagnosis is to know the patient’s voice disorder history. Social impact of voice problem on the child, communication problems with the environment, quality of life, personal development and academic activities (such as school success) should be evaluated in the patient’s history. Examination of the vocal cords by an Otolaryngologist is the second step of the diagnosis after the history. The presence of a pathology that can be detected in the examination is important in terms of directing the treatment. If possible, recording the child’s voice and examining it through special computer programs will also help in the diagnosis. There is also a group of patients whose examination is completely normal, including the vocal cords during ENT examination. It should not be forgotten that some psychological reasons such as anxiety, depression and personality disorders may cause hoarseness in these patients and the treatment plan should be developed in this direction.
How should childhood voice problems be treated?
Etiology is important in the treatment of hoarseness in children. The fact that some measures that should be taken along with the family and at home enviroment for vocal health and hygiene, both facilitates the treatment and prevents recurrence of the disease. The treatment plan to be made according to the reason includes sometimes surgery, sometimes medication, sometimes psychotherapy and often voice therapy. Psychotherapy support should be provided especially for voice problems due to behavioral disorders (frequent crying, shouting, peevish children, etc.). In the practice of voice therapy, the child is tried to be aware of his / her voice and speech behaviors, and therapy methods are applied that will enable the child to recognize and correct his/her negative behaviors.
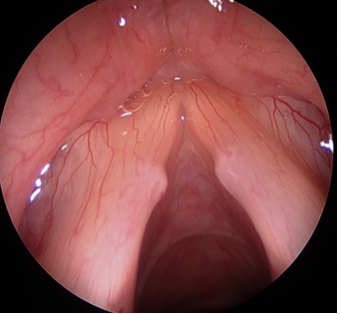
The most common cause of hoarseness in children is nodules. Nodules are symmetrically shaped calluses that occur in the anterior parts of both vocal cords. They prevent the vocal cords to close completely during speech and thus the quality of the voice deteriorates. Treatment in nodules should primarily be in the form of vocal hygiene, voice and behavioral therapy (a therapy integrity including psychotherapy should be provided to improve speech habits). Surgical treatment should be postponed as much as possible and time should be gained with the expectation that the child’s speech habits will improve in a positive way and the nodule may regress in this way. If other treatments do not work, removal of the nodule under general anesthesia can be thought as the last treatment method.
Diseases such as polyps and cysts are much less common in pediatric vocal cords than nodules, and in the treatment, similar measures should be taken at the beginning and then a surgical treatment plan should be made if it is necessary.
If there is a hoarseness due to stomach acid reflux in children, the regulation of eating habits and drug treatment should be first.
The problem of vocal cord paralysis or weakness in vocal cord movements may affect the vocal cord unilaterally or bilaterally. These may be congenital or may occur due to a trauma during birth. In addition some cardiological, neurological, tumoral, unknown causes or infections may cause to the vocal cord paralysis in postpartum period. Complaints in vocal cord paralysis are different when it is unilateral or bilateral, and this situation affects directly the treatment plan (See: Treatment in vocal cord paralysis). The formation of web in the vocal cord, which is usually congenital in childhood, but may also appear later as a result of some surgical interventions on the vocal cord, mostly affects the anterior 1/3 of the vocal cords. The treatment is to open web formation surgically (with laser or cold knife).
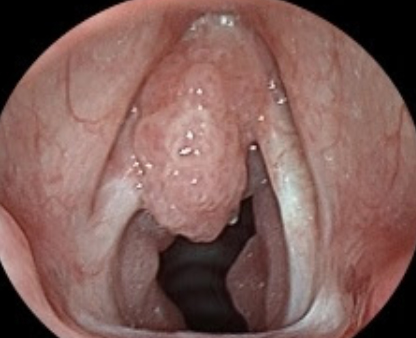
Benign tumors, also called papillomatosis or juvenile laryngeal papillomatosis, are the most common tumoral lesions in childhood and are more troublesome than their adult form. The main problem in these children is hoarseness and breathing difficulty that develops as the mass grows and narrows the airway. Human papillomavirus (HPV) is the causative microorganism in the disease and HPV Type 6 and 11 are the most common in laryngeal papillomatosis. In the examination, masses like cauliflower are seen on the vocal cords and it sometimes also extends to the surrounding tissues. As a precaution, vaccination is recommended for the risky HPV types in childhood. In surgical treatment, the tissue is removed under general anesthesia microscopically and by using LASER. These tumors are prone to recurrence and may require multiple surgical procedures.
In the treatment of functional voice problems (such as muscle tension dysphonia, puberphonia, psychogenic dysphonia), the coordination of the muscles that contribute to the work of the vocal cord is provided by means of psychotherapy, behavioral therrapy and voice therapy.
In this group, especially puberphonia (mutational falsetto) will be emphasized. Especially in boys, it is a situation that occurs when the child cannot accept the voice they hear and tries to use his old childish voice due to the sudden deepening of the voice during adolescence. The use of such a voice is contrary to the natural functioning of the vocal cords, and it turns into a shape that does not fit any voice format (neither child, nor girl, nor male voice), in the form of high pitched and thinning.It is usually seen in the 11-16 age group, but if it is not treated, the problem continues towards later ages and may be permanent. If this voice disorder is not treated in a timely manner, it affects the child’s school success, psychology and career plans in adulthood negatively. The treatment of these patients is possible with voice therapy. In this treatment, the patient is taught how to use the laryngeal muscles and what his / her own natural voice should be and is encouraged to use this voice.


